Signed in as:
filler@godaddy.com
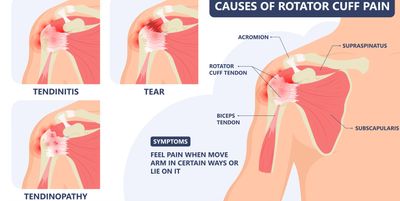
Rotator cuff tears are a common disorder of the shoulder. Many patients, 50% over 60 years of age may have rotator cuff tear. Many of these tears are partial, asymptomatic, but many are causes of pain and loss of function. The four main muscles and their associated tendons of the rotator cuff are, Subscapularis muscle, Supraspinatus muscle, Infraspinatus muscle, Teres Minor muscle. A tear or part, one or several of these tendons causes different pain and symptoms.
Tendon tears occur from different causes, the common cause of tendon degeneration, and less common cause of trauma related. These two aetiologies are treated slightly different with timing of surgery and possible repair options. Dr Drynan will go through your case in detail with you at your consultation. Degeneration of the tendon, approximately 3-4mm from its insertions to the humerus due to a mismatch in repair and degeneration of the tendon. There are intrinsic causes, such as genetics, medical conditions and others and extrinsic causes, such as muscle imbalance and over use injuries.
The most common symptoms are pain, located over the deltoid and upper arm. This can be a of other shoulder pathology as well, as shoulder pain is often poorly localised. Larger rotator cuff tears often lead to weakness and lack of function for the shoulder or fatigue of the shoulder with repetitive or over head activities.
Diagnosis is based on your history, examination and investigations. Gold standard non invasive investigation of choice is MRI. This is a non radiation imaging modality that allows good imaging for the rotator cuff, cartilage, bones, bursa, tendons and around the shoulder. This imaging requires involves the use of strong magnetic field manipulation to obtain the imaging, thus may not be for everyone such as those with pacemakers, nerve stimulators and other causes, but speak to your imaging provider. Ultrasounds can be used when MRI is contraindicated, but imaging quality and other diagnostic power is not as thorough as with an MRI.
Management of rotator cuff tears includes non operative and operative treatments, with the ultimate goal of improving your shoulder pain and function.
Non-operative management may include:
Operative management aims are to restore the tendon back to the anatomic insertion point, under physiologic stress (normal tension) and achieve healing. There are many steps involved to achieve this.
Occasionally anatomic tendon repairs may not be possible. If this is the case, Dr Drynan will discuss other evidence based treatments that may assist in your shoulder treatment, such as superior capsule reconstruction, tendon transfers, and arthroplasty.
If surgery is the right choice for you, then understanding the surgery is beneficial. There are a few main considerations with surgical interventions.
Decision for operation:
Operation:
Pain control:
Rehabilitation and recovery time:
Post injury and post surgical rehabilitation is often beneficial. Many studies have assessed in home, remote and in person physical therapy following rotator cuff surgery and total shoulder replacement. Although the results are mixed to show a large benefit from in-person rehab, Dr Drynan still recommends some guidance by a Physiotherapist. To assist the rehabilitation process Dr Drynan has a protocol for you on your day of surgery and a downloadable document on the patient information page to guide home exercises following your shoulder surgery.